University of Wisconsin School of Medicine and Public Health Madison, WI
Award: Presidential Poster Award
Dana Ley, MD1, Saqib Walayat, MD1, Kusum Sharma, MBBS1, Mark Albertini, MD1, Rashmi Agni, MD1, Deepak Gopal, MD, FACG2 1University of Wisconsin School of Medicine and Public Health, Madison, WI; 2University of Wisconsin School of Medicine, Madison, WI
Introduction: Gastroenterologists are consulted on immune checkpoint inhibitor (ICI)-related adverse events, most commonly diarrhea, colitis, and hepatotoxicity. ICI-related or type III autoimmune pancreatitis (AIP) is uncommon and presents unpredictably. Lipase elevations and clinical pancreatitis may occur without imaging findings of AIP. We present a case of type III AIP; to our knowledge, the first biopsy-proven case described.
Case Description/Methods: A 71-year-old male with metastatic mucosal melanoma of the urethra (on palliative nivolumab/relatlimab) complicated by adrenal insufficiency and microscopic colitis developed vague epigastric discomfort and elevated amylase and lipase (< 5x upper limit of normal [ULN]) after cycle 4, further increasing after cycle 5 (lipase >20x ULN). ICI was held. Abdominal CT 1 month later showed prominent pancreatic duct (PD) without clear mass. PET scan showed decreased metastatic inguinal lymph node uptake. Three months after his ICI was held, the amylase and lipase remained elevated and started to up-trend. CT abdomen/pelvis with contrast showed infiltrative pancreatic masses. IgG4 level was normal.
EUS-FNBx showed two irregular-appearing masses in the pancreatic head and distal body, with upstream PD dilation. Pathology of the pancreatic head mass showed patchy pancreatitis with acinar lymphocyte-rich inflammation. Pathology of the distal mass showed atrophic tissue with lymphocyte-rich stromal inflammation, ductitis and venulitis in an “immune injury” pattern. There was no evidence of malignancy. The findings were felt consistent with ICI-related type III AIP.
The patient developed progressive, severe abdominal and back pain, fever, chills, and nausea post-EUS and was admitted three days later for acute pancreatitis. He was treated symptomatically and started on prednisone 40 mg daily for type III AIP, with plans for a slow taper. His symptoms resolved, and his amylase and lipase improved. Recent PET CT showed no evidence of FDG-avid residual or recurrent malignancy.
Discussion: Type III AIP incidence is low, likely ≤1%, without clear temporal relationship to ICI initiation or cessation. Usually diagnosed clinically, it may have an atypical presentation. Given the infiltrative masses on abdominal CT, our patient had an EUS-FNBx. Given his history, there was concern for either melanoma metastases or primary pancreatic adenocarcinoma, so the biopsy changed management. This is the first reported case describing pathology findings of type III AIP diagnosed by EUS-FNBx.
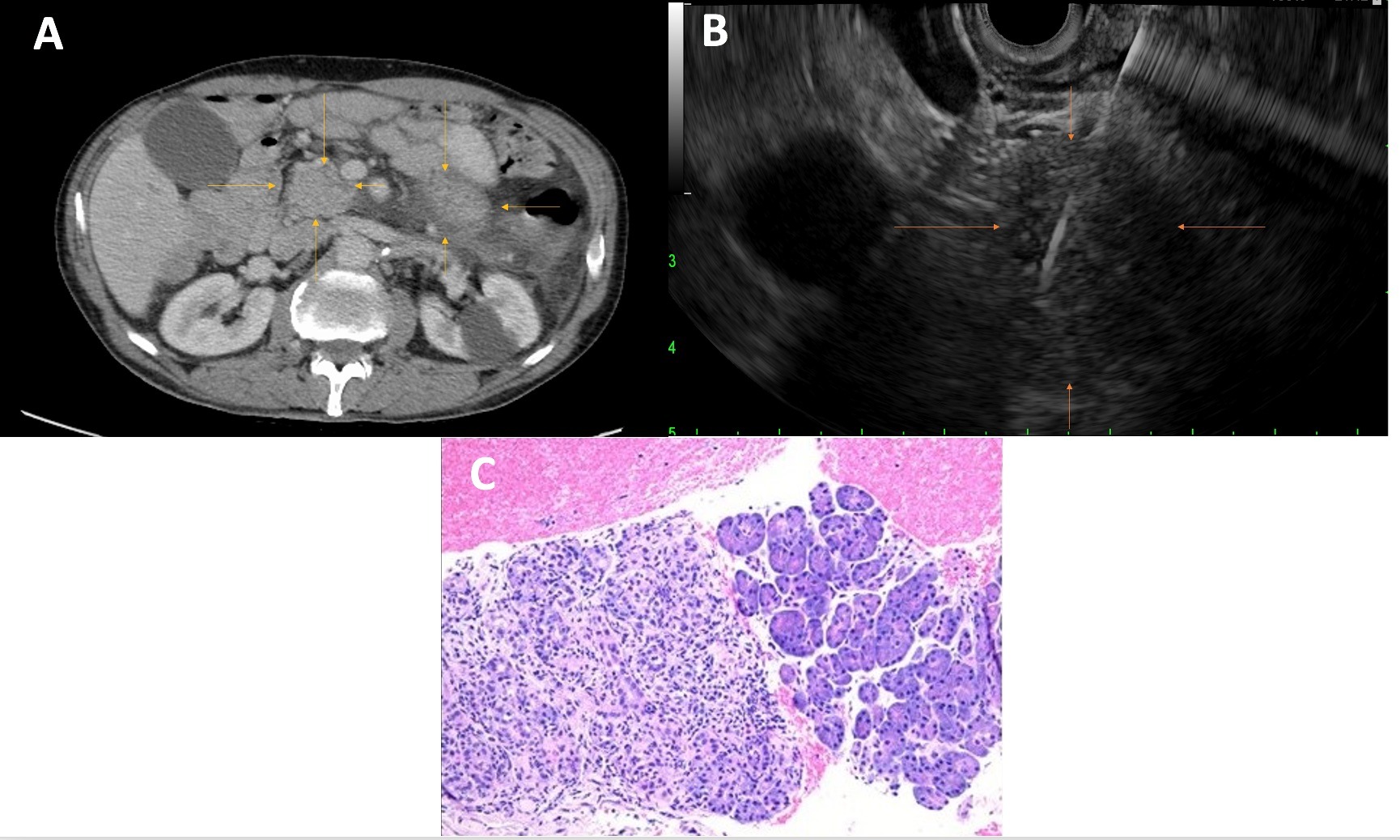
Figure: Panel A: Axial CT of the abdomen/pelvis with contrast with arrows indicating infiltrative masses in the pancreatic head and distal body/tail. Panel B: Endoscopic ultrasound with fine needle biopsy image showing irregular oval mass in the pancreatic head (indicated by arrows), measuring 30 mm x 18 mm in maximal cross-sectional diameter with irregular outer margins. Fine needle biopsy 22-gauge core needle is seen entering the mass. Panel C: Hematoxylin and Eosin stained-pathology slide showing pancreatic acinar structures infiltrated with lymphocyte-predominant, mixed inflammatory infiltrates, with acinar damage and dropout.
Disclosures:
Dana Ley indicated no relevant financial relationships.
Saqib Walayat indicated no relevant financial relationships.
Kusum Sharma indicated no relevant financial relationships.
Mark Albertini: Apeiron Biologics – Advisor or Review Panel Member. Array BioPharma Inc. – Advisor or Review Panel Member. Bristol-Myers Squibb Company – Advisor or Review Panel Member. Merck & Co., Inc. – Advisor or Review Panel Member. Nektar Therapeutics – Advisor or Review Panel Member.
Rashmi Agni indicated no relevant financial relationships.
Deepak Gopal indicated no relevant financial relationships.
Dana Ley, MD1, Saqib Walayat, MD1, Kusum Sharma, MBBS1, Mark Albertini, MD1, Rashmi Agni, MD1, Deepak Gopal, MD, FACG2. P2908 - Endoscopic Ultrasound With Fine Needle Biopsy Confirming a Diagnosis of Immune Checkpoint Inhibitor-Related Type III Autoimmune Pancreatitis, ACG 2023 Annual Scientific Meeting Abstracts. Vancouver, BC, Canada: American College of Gastroenterology.