The Warren Alpert Medical School of Brown University Providence, RI
Kuntal Bhowmick, MD1, Breton Roussel, MD1, J Filipe Monteiro, PhD2, Kanwal Bains, MBBS, CNSC3, Mouhand Mohamed, MD4, Neha Wadhavkar, MD4, Markos Kalligeros, MD1, Sean Fine, MD, MS5 1Warren Alpert Medical School of Brown University, Providence, RI; 2Brown Medicine/Lifespan, Providence, RI; 3University of Arizona, Tucson, AZ; 4Brown University, Providence, RI; 5Warren Alpert Medical School of Brown University, Providence, RI
Introduction: Esophageal food impaction (EFI) is a common gastrointestinal complaint, often prompting presentation to the emergency department (ED) and requiring esophagogastroduodenoscopy (EGD) for disimpaction. Methods for procedural sedation include moderate sedation (MS) or anesthesia administered sedation (AAS), which refers to monitored anesthesia care and general anesthesia. Endoscopy staff typically administers MS, but this may be burdensome to the endoscopist managing a potentially emergent condition. We aimed to evaluate differences in case duration with EFI interventions under MS versus AAS and their clinical implications.
Methods: We conducted a retrospective review of 554 adult patients who presented to the ED with suspected EFI at the 3 Lifespan academic or community hospital sites from 2015 to 2021. Forty-five patients were excluded for absence of EFI on EGD. We compared procedure time (“scope in” and “scope out”) and sedation duration by MS versus AAS. Procedure and sedation durations were also compared by Charlson Comorbidity Index (CCI) and rate of complications (perforation, aspiration, esophageal ulceration, surgical intervention). Chi-square, Fisher exact test, and Student’s t-tests were performed for descriptive analysis to report demographics and other health-related measurements. Analysis was performed in SAS version 9.4.
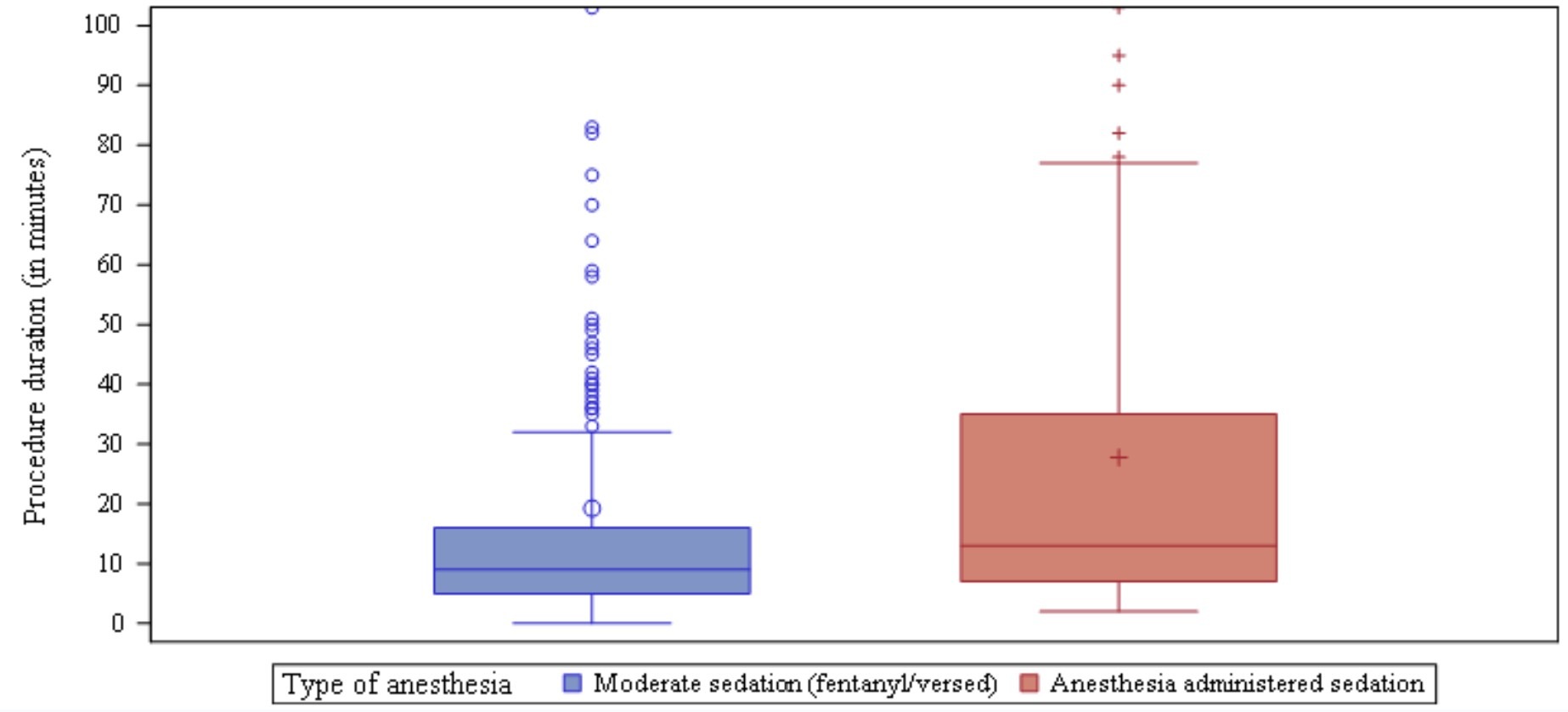
Results: The main significant finding was a lower average sedation duration under MS (93.4±165.2 minutes) versus AAS (176.1±541.8) (p=0.0423). The average procedure duration was not statistically significant (MS 19.3±90.2 versus AAS 27.8±36.1; p=0.1758). Further findings that did not reach statistical significance are as follows: procedures with at least 1 complication had average procedure and sedation durations of 32.1±30.5 and 338.4±635.5, compared to no complications at 22.1±75.8 (p=0.2657) and 117.7±346 (p=0.1867), respectively. Average procedure and sedation duration among individuals with CCI >2 was 26.0±30.8 and 194.7±658.0, compared with individuals with CCI ≤ 2 at 21.6±81.7 (p=0.4367) and 108.9±245.6 (p=0.2213), respectively.
Discussion: In this multisite cohort study, we found no association between overall procedure duration in MS versus AAS, despite a lower sedation time under MS. Furthermore, comorbidity burden was not demonstrated to impact procedural or sedation duration, and neither procedural nor sedation duration were associated with complication rates.
Figure: Procedure duration by moderate sedation (midazolam & fentanyl) and anesthesia administered sedation (monitored anesthesia care or general anesthesia)
Disclosures:
Kuntal Bhowmick indicated no relevant financial relationships.
Breton Roussel indicated no relevant financial relationships.
J Filipe Monteiro indicated no relevant financial relationships.
Kanwal Bains indicated no relevant financial relationships.
Mouhand Mohamed indicated no relevant financial relationships.
Neha Wadhavkar indicated no relevant financial relationships.
Markos Kalligeros indicated no relevant financial relationships.