Mohammad A. Ahmed-Khan, MD1, Nisha Nepal, MD2, Nkechi Okam, MD2 1Danbury Hospital - Yale School of Medicine, Danbury, CT; 2Danbury Hospital, Danbury, CT
Introduction: Imatinib is an oral chemotherapeutic agent that inhibits tyrosine kinases such as BCR-ABL, c-KIT and is commonly used for Philadelphia chromosome-positive chronic myelogenous leukemia (CML) and c-KIT gastrointestinal stromal tumors (GIST). Imatinib has various side effects, including rash, pancytopenia, hypothyroidism, cardiac, renal, and liver toxicity. We report a case of a 53-year-old woman with a recent diagnosis of locally advanced GIST on Imatinib who presented with acute liver failure who returned to her baseline status after discontinuation of imatinib and initiation of prednisolone.
Case Description/Methods: A 53-year-old woman with history of beta-thalassemia and recently diagnosed locally advanced GIST complicated by contained perforation and hepatic abscess status post partial gastrectomy and Billroth II gastrojejunostomy, status post partial right-sided hepatectomy and on imatinib therapy on and off for 5 months presented with weakness, anorexia, weight loss. Her liver function tests showed aspartate aminotransferase (AST) 1309 U/L, alanine transaminase (ALT) 942 U/L, gamma-glutamyl transferase (GGT) 111, Alkaline phosphatase (ALP) 131, direct bilirubin 9.8 mg/dl, total bilirubin 15.2 mg/dl, INR 1.82. Cat scan abdomen and pelvis showed status post partial gastrectomy and Billroth II gastrojejunostomy, status post partial right-sided hepatectomy, and newly evident periportal edema. MRCP showed gastric and partial right lobe hepatic resections as well as cholecystectomy, unchanged mild to moderate splenomegaly. Autoimmune and viral hepatitis panel were negative with ANA < 1:40, anti-mitochondrial and anti-smooth muscle antibody negative, EBV, CMV, Hepatitis B, C, A negative. Urine toxin was unremarkable. The patient underwent liver biopsy, which showed cholestatic hepatitis with bridging necrosis. Imatinib was discontinued, and she was started on prednisolone 40mg/day with a slow taper. Her liver function test gradually improved to AST/ALT 32/28, ALP 92, and total bilirubin 1.5 in a couple of months. She is currently following up with her oncologists for alternative GIST treatment options.
Discussion: In conclusion, although imatinib is generally well-tolerated, it is important to monitor patients for potential side effects, including severe hepatotoxicity. Early recognition of imatinib-induced fulminant hepatitis and immediate administration of prednisolone or prednisone can be lifesaving and prevent the need for liver transplantation.
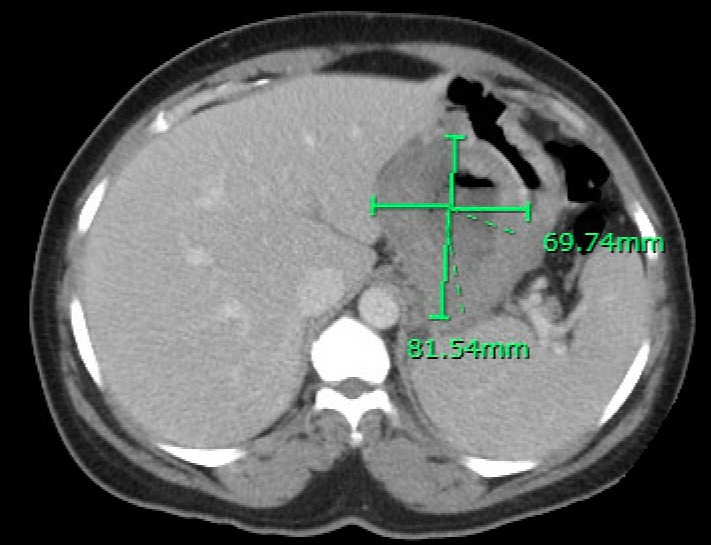
Figure: Findings compatible with fungating gastric malignancy measuring up to 8 cm in diameter.
Disclosures:
Mohammad Ahmed-Khan indicated no relevant financial relationships.
Nisha Nepal indicated no relevant financial relationships.
Nkechi Okam indicated no relevant financial relationships.
Mohammad A. Ahmed-Khan, MD1, Nisha Nepal, MD2, Nkechi Okam, MD2. P1002 - Imatinib-Induced Fulminant Hepatitis: A Case Report and Literature Review, ACG 2023 Annual Scientific Meeting Abstracts. Vancouver, BC, Canada: American College of Gastroenterology.