Shazia Rashid, MD, Daniyal Raza, MD, Omar Khan, MD, Hassaan A. Zia, MD LSU Health Sciences Center, Shreveport, LA
Introduction: Esophageal leukoplakia is a premalignant lesion with a potential to progress into squamous cell carcinoma. The prevalence of leukoplakia in a group of 1048 patients who underwent esophageal biopsies for various indications was found to be 0.19%, indicating its rarity. It can present as dysphagia but often is an incidental finding. We present a case of a patient with recurrent strictures secondary to esophageal leukoplakia.
Case Description/Methods: A 70-year-old woman with a history of sarcoidosis on oral steroids, prior oral Human Papilloma Virus (HPV) lesions who presented with a 6-month history of solid food and liquid dysphagia. She denied nausea, emesis, abdominal pain, weight loss, history of allergies, asthma, smoking or alcohol use. She underwent multiple esophagogastroduodenoscopies (EGDs), which showed two strictures at 20cm and 35cm from incisors, requiring repeat dilations. It also showed patchy white plaques throughout the esophagus and biopsies during the fourth EGD showed fungal elements. Pt was treated with fluconazole and reported mild improvement in symptoms. Per discussion with pulmonology, steroids were discontinued given increased risk of candidiasis. During subsequent EGD, two dominant strictures were again visualized with overlying whitish plaques. Biopsies from the strictures showed esophageal mucosa with hyperkeratosis and prominent granulosa cell layer (epidermoid metaplasia) favoring esophageal leukoplakia, no fungal elements were seen. Random esophageal biopsies also showed acute esophagitis and increased intraepithelial eosinophils (up to 25 per high-power field). Pt was started on topical swallowed fluticasone and scheduled for repeat EGD for dilation.
Discussion: Esophageal leukoplakia is a rare condition associated with esophageal squamous cell carcinoma. It is commonly seen in middle-aged adults with a history of alcohol or tobacco abuse. HPV is a risk factor for oral leukoplakia; however no association has been found with esophageal leukoplakia. Although seen incidentally in many cases, esophageal metaplasia may present with dysphagia. Endoscopically, esophageal leukoplakia appears as a white plaque that cannot be easily scraped off, consistent with our patient's findings. Treatment options depend on the size and resectability of the lesion, with endoscopic resection suitable for smaller lesions and ablation therapy considered for larger lesions with dysplasia. Currently, there are no established guidelines for post-ablation surveillance in cases of leukoplakia.
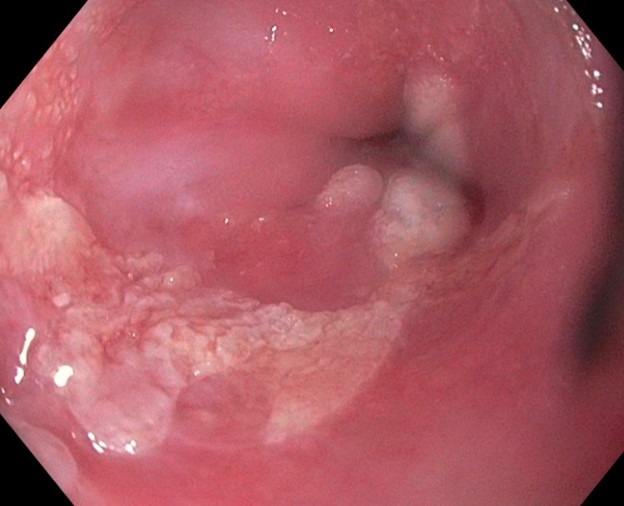
Figure: Patchy white plaques seen in esophagus on EGD examination consistent with esophageal leukoplakia
Disclosures:
Shazia Rashid indicated no relevant financial relationships.
Daniyal Raza indicated no relevant financial relationships.
Omar Khan indicated no relevant financial relationships.
Hassaan A. Zia indicated no relevant financial relationships.
Shazia Rashid, MD, Daniyal Raza, MD, Omar Khan, MD, Hassaan A. Zia, MD. P3334 - Esophageal Leukoplakia: A Rare Cause of Esophageal Stricture, ACG 2023 Annual Scientific Meeting Abstracts. Vancouver, BC, Canada: American College of Gastroenterology.