Rabia Rizwan, MD1, Waseem Amjad, MD2, Paul Feuerstadt, MD, FACG3, AbdelKader Chaar, MD1, Ahmad Nawaz, MD1, Karthik Gnanapandithan, MD4, Abdul Q. Bhutta, MD5, Marc Fenster, MD6, Savio John, MD7, Kanika Sehgal, MBBS8, Lawrence Brandt, MD, MACG9 1Yale University School of Medicine, New Haven, CT; 2Brockton Hospital, Brockton, MA; 3PACT Gastroenterology Center and Yale School of Medicine, Hamden, CT; 4Mayo Clinic Florida, Jacksonville, FL; 5University Gastroenterology, Portsmouth, RI; 6Montefiore, Bronx, NY; 7SUNY Upstate Medical University, Syracuse, NY; 8Yale-New Haven Hospital, New Haven, CT; 9Montefiore Medical Center, Bronx, NY
Introduction: Colon Ischemia (CI) manifests a range of severity from reversible to fulminant disease requiring colectomy or resulting in death. Our goal was to develop a 30-day prediction score to triage the risk of progression of severe disease to colectomy or mortality in patients hospitalized with CI.
Methods: A multicenter retrospective study of patients hospitalized with biopsy-proven CI from 1/2005 to 7/2017. Patients with age < 45 yrs, the extreme elderly ( > 90 yrs), and those with colon cancer were excluded. Patients requiring colectomy and/or dying within 30 days of presentation were classified as having severe disease. A multivariable Cox-proportional hazard model was used to identify risk factors for severe CI. Beta coefficients of independent risk factors were used to generate the scoring system. Coefficients were rounded to the nearest decimal value multiple of 0.25 to generate a Clinically Applicable Prognostication Severity Score for CI (CAPSSCI). We calculated area under receiver operating curve (AUROC) of predicted and observed severe CI.
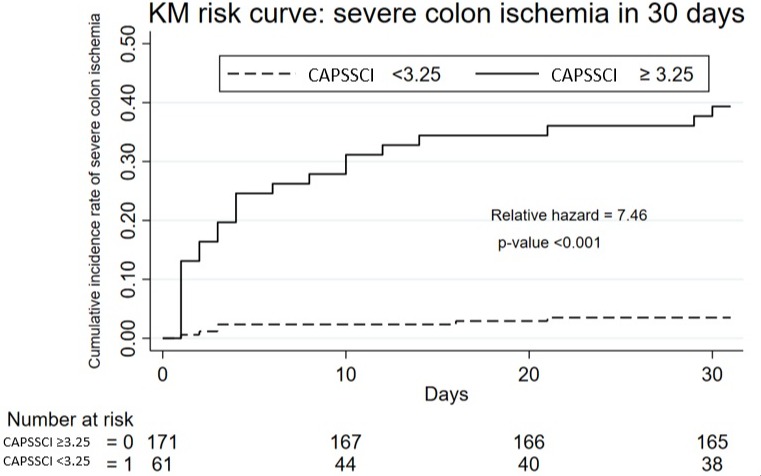
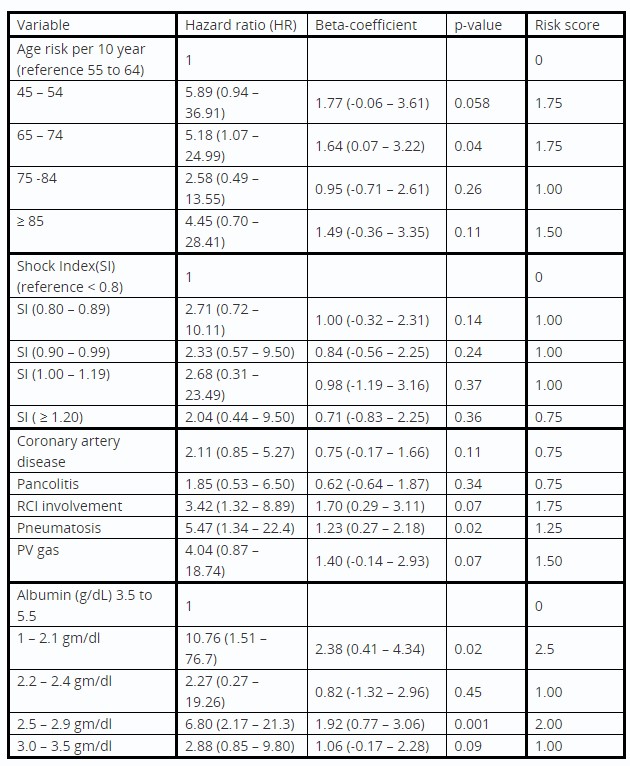
Results: 713 pts with biopsy-proven CI met study criteria. Of these, 82 (11.3%) developed severe CI within 30 days of presentation. Their mean age was 70.1 ± 10.9 yrs, and 74.7% were male. The severe CI group had a higher percentage of women (41.5 vs. 23.3, p=0.001), coronary artery disease(CAD; 46.3 vs. 31.0, p=0.007) and COPD (18.3 vs. 9.8, p=0.030). The multivariable model showed the following to be associated with severe CI: ages 45 to 54 yrs and advanced age (compared to reference: 55 to 64 yrs); CAD (HR: 3.01, 95% CI: 1.10 – 8.30, p=0.03), shock index (HR: 5.65, 95% CI: 1.11 – 28.8, p=0.04), lower albumin, imaging findings of pan-colon and right-colon involvement, pneumatosis, and portal venous gas. A 45-point score (0 to 11.25 with 0.25 increment) CAPSSCI was generated using point estimates (β) of these risk factors. (Table 1) AUROC to predict severe CI was 0.90 (95% CI: 0.85 – 0.93) at 30 days, and 5-fold internal cross-validation AUROC to predict 30-day severe CI was 0.87 (95% CI: 84 – 0.94). A cut-off of 3.25 accurately calibrated the risk for severe CI (sensitivity = 80.65%, 95% CI: 75.57% – 85.72% and specificity= 81.68%, 95% CI: 76.72% – 86.65%). (Figure 1)
Discussion: CAPSSCI is a simple-to-use risk score integrating baseline clinical variables and available diagnostic data. Healthcare providers can use this calculation to easily assess risk for severe outcomes of CI in hospitalized patients and direct therapy based upon this risk
Figure: Kaplan-Meier (KM) Risk Curve showing the incidence of severe colon ischemia with Clinically Applicable Prognostication Severity Score for Colon Ischemia (CAPSSCI) ≥ 3.25 and for CAPSSCI < 3.25 in 30-day follow-up
Table: Components of Clinically Applicable Prognostication Severity Score for Colon Ischemia (CAPSSCI): Variables included in the model are age, history of coronary artery disease (CAD), lower albumin level, shock index (ratio of heart rate and systolic blood pressure) and imaging findings including pancolitis, right colon Ischemia (RCI) Involvement, pneumatosis, and portal venous (PV) gas.
Disclosures:
Rabia Rizwan indicated no relevant financial relationships.
Waseem Amjad indicated no relevant financial relationships.
AbdelKader Chaar indicated no relevant financial relationships.
Ahmad Nawaz indicated no relevant financial relationships.
Karthik Gnanapandithan indicated no relevant financial relationships.
Abdul Bhutta indicated no relevant financial relationships.
Marc Fenster indicated no relevant financial relationships.
Savio John indicated no relevant financial relationships.
Kanika Sehgal indicated no relevant financial relationships.
Lawrence Brandt: Ferring Pharmaceuticals – Advisor or Review Panel Member, Consultant.
Rabia Rizwan, MD1, Waseem Amjad, MD2, Paul Feuerstadt, MD, FACG3, AbdelKader Chaar, MD1, Ahmad Nawaz, MD1, Karthik Gnanapandithan, MD4, Abdul Q. Bhutta, MD5, Marc Fenster, MD6, Savio John, MD7, Kanika Sehgal, MBBS8, Lawrence Brandt, MD, MACG9, 12, Development of a Clinically Applicable Prognostication Severity Score for Colon Ischemia in Hospitalized Patients, ACG 2023 Annual Scientific Meeting Abstracts. Vancouver, BC, Canada: American College of Gastroenterology.