10 - Association Between Cold Snare Polypectomy Rate (CSPR) and Existing Endoscopist Quality Metrics: A New Frontier in Colonoscopy Quality Measurement?
Award: Outstanding Research Award in the Colorectal Cancer Prevention Category
Seth D. Crockett, MD, MPH1, Rajesh Keswani, MD, MS2, Audrey H.. Calderwood, MD, MS3, Jennifer Holub, MPH4 1Oregon Health & Science University, Portland, OR; 2Northwestern University Feinberg School of Medicine, Chicago, IL; 3Dartmouth Health, Lebanon, NH; 4GI Quality Improvement Consortium, Ltd., Bethesda, MD
Introduction: Colon polypectomy is essential to the prevention of colorectal cancer, but polypectomy quality is variable in practice. Recent guidelines recommend use of cold snares for removal of most polyps < 1 cm. However, colonoscopist adherence to these recommendations, and the extent which polypectomy practice correlates with existing quality metrics is unknown.
Methods: We selected complete colonoscopies with one or more small ( < 1 cm) polyp removed among screening and surveillance colonoscopies in patients aged 40-80 in the GIQuIC registry between 2019-2022. Procedures with larger polyps or cancer, diagnostic exams, and inadequate bowel prep were excluded. Polypectomy technique was determined, and the cold snare polypectomy rate (CSPR) was calculated for each endoscopist with at least 50 colonoscopies, and available data on adenoma detection rate (ADR), withdrawal time (WT), and cecal intubation rate (CIR). Other endoscopist factors included specialty, practice location, annual colonoscopy volume, and serrated polyp detection rate (SDR). Bivariate proportions were compared by Chi-squared tests, and multivariable analysis was performed using logistic regression.
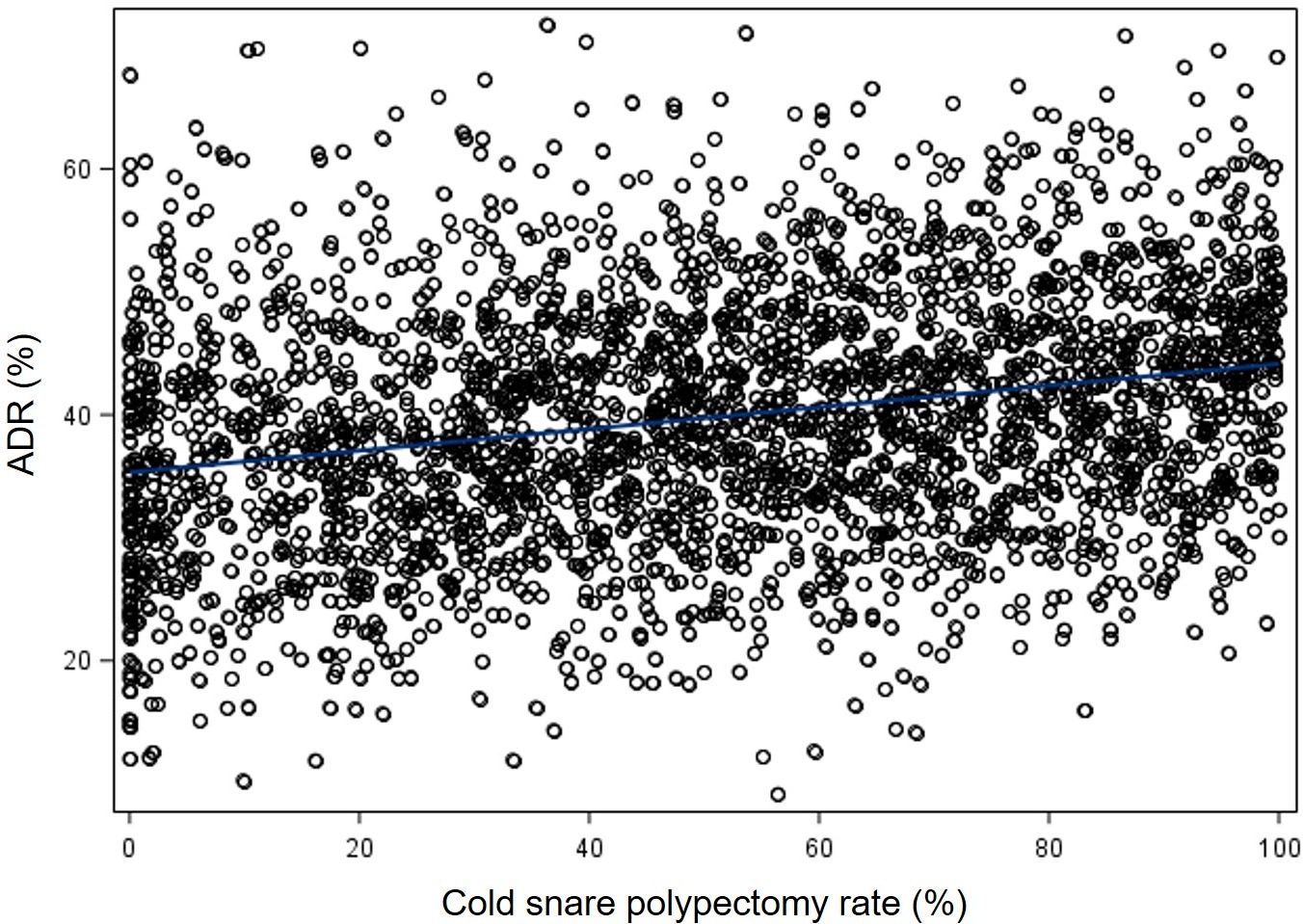
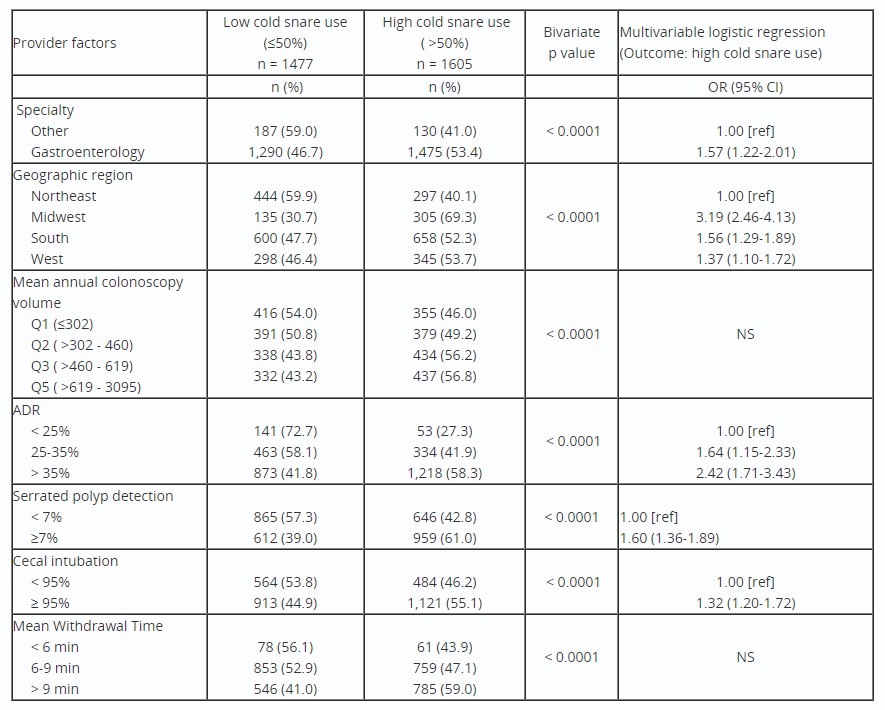
Results: A total of 1,589,499 colonoscopies were done in patients with 1 or more small polyps removed. Among the performing endoscopists, 3,082 met the inclusion criteria and were included in the analysis. The mean endoscopist CSPR (± SD) was 51.2 (±29.2). We found that higher CSPR ( >50%) was associated with GI specialty training, geographic region (highest in Midwest: 69%; lowest in Northeast: 40%), and colonoscopy volume (10 percentage points higher for Q4 vs Q1) (all p < 0.0001) (Table). Regarding quality metrics, the CSPR was over 30 percentage points higher for those with ADR >35% compared to those with ADR < 25% (58% vs 27%, p < 0.0001) (Figure). Higher endoscopist SDR, CIR and WT were also associated with higher CSPR (all p < 0.0001). On multivariable analysis, we found that higher ADR, SDR, CIR, GI specialty, and region were all independently associated with higher CSPR.
Discussion: Cold snare usage for removal of small polyps was lower than expected based on current guideline recommendations. Higher CSPR was most strongly associated with geographic location, GI specialty, and higher performance on existing quality metrics of ADR, SDR, and CIR. We demonstrate that CSPR can be measured using registry data, and is another possible tool for use in quality improvement for screening colonoscopy.
Figure: FIGURE: Scatter Plot of ADR and Cold Snare Polypectomy Rate Among Endoscopists in GIQuIC for Colonoscopies with <1cm Polyps
Table: TABLE: Bivariate and Multivariable Analysis of Endoscopist-level Predictors of Cold Snare Usage for Polyps <1cm (n = 3,082 endoscopists, GIQuIC 2019-2022). To be included in the study, endoscopists had to have a minimum of 50 procedures where a small polyp was removed and have valid quality measure data. ADR: adenoma detection rate; OR: odds ratio; CI: confidence interval; NS: not significant.
Rajesh Keswani: Boston Scientific – Consultant. Medtronic – Consultant.
Audrey Calderwood: Dark Canyon Laboratories – Advisory Committee/Board Member.
Jennifer Holub indicated no relevant financial relationships.
Seth D. Crockett, MD, MPH1, Rajesh Keswani, MD, MS2, Audrey H.. Calderwood, MD, MS3, Jennifer Holub, MPH4, 10, Association Between Cold Snare Polypectomy Rate (CSPR) and Existing Endoscopist Quality Metrics: A New Frontier in Colonoscopy Quality Measurement?, ACG 2023 Annual Scientific Meeting Abstracts. Vancouver, BC, Canada: American College of Gastroenterology.




 photo")