Pradeep Koripella, MD1, Eshandeep Boparai, MD1, Christopher Jensen, PhD, MPH1, Jessica Badalov, MS, RDN1, Charles Quesenberry, PhD1, Sophia Merchant, MPH1, Theodore R. Levin, MD2, Jeffrey Fox, MD1, Douglas Corley, MD, PhD1, Jeffrey Lee, MD, MPH3 1Kaiser Permanente, San Francisco, CA; 2Kaiser Permanente, Oakland, CA; 3Kaiser Permanente San Francisco Medical Center, San Francisco, CA
Introduction: Recent guidelines have recommended that patients with low-risk adenomas receive a follow-up colonoscopy in 10 years rather than 5 years. Faced with these updated guidelines, a challenge to healthcare systems is how to de-implement outdated surveillance recommendations for low-risk patients who have a 5-year follow-up interval and transition them to the recommended 10-year interval.
Methods: We conducted a 3-arm, pragmatic, randomized trial comparing three outreach interventions for adopting the new 10-year surveillance interval recommendation. Members from an integrated health center were eligible for the trial if they were average-risk adults 54-70 years of age who underwent a baseline colonoscopy with 1-2 small tubular adenomas between 2017 and 2018 and were coming due for their 5-year surveillance procedure.
The intervention included three outreach approaches (secure messaging, telephone, and mailed letter). The messaging content was identical across all three group in explaining that patients were eligible to extend their prior surveillance interval from 5 to 10 years. Patients were provided the following response options: 1) adopt the 10-year surveillance interval recommendation or 2) continue with the prior 5-year surveillance recommendation. All patients were given an opportunity to request an appointment with their physician to have a shared decision-making approach.
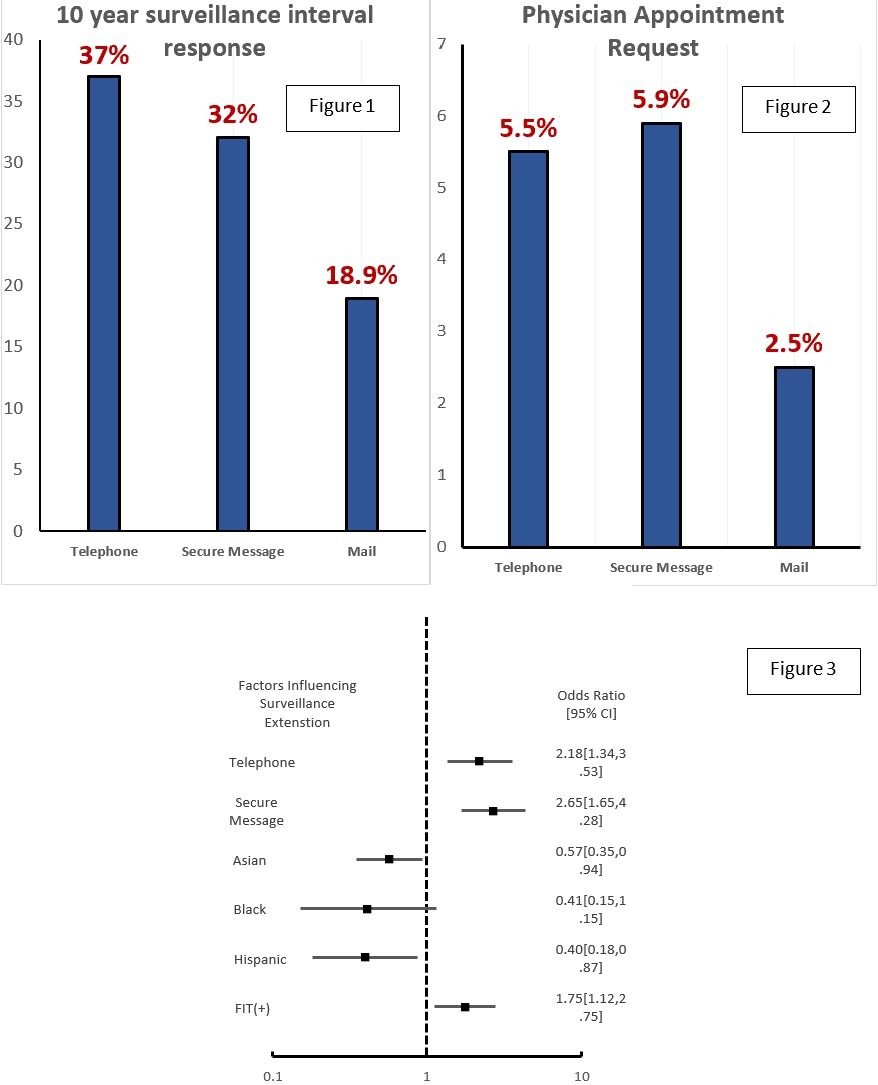
Results: 37% of participants in the telephone group, 32% in the secure message group, and 18.9 % in the mail group chose to extend surveillance. (p< 0.001, Figure 1). Requests for shared decision-making with a physician ranged from 2.5%-5.9% as shown in Figure 2. Factors influencing surveillance extension are noted in Figure 3. The black cohort did not reach significance likely due to the size of the cohort.
Discussion: In this clinical trial we demonstrated that patient outreach to de-implement outdated recommendations is feasible. Telephone outreach was the most effective followed by secure messaging. Minority groups were less likely to extend surveillance, which suggests a possible gap in culturally component care. (+)FIT test prior to colonoscopy was a factor that had increased odds of changing surveillance time, suggesting a difference in patient preference regarding screening colonoscopy. To our knowledge, this marks the first implementation of patient outreach to de-implement outdated recommendations.
Figure: Figure 1: Percentage of surveillance extension per group Figure 2: Rates of physician appointment request Figure 3: odds ratio of various factors influencing surveillance extension
Disclosures:
Pradeep Koripella indicated no relevant financial relationships.
Eshandeep Boparai indicated no relevant financial relationships.
Christopher Jensen indicated no relevant financial relationships.
Jessica Badalov indicated no relevant financial relationships.
Charles Quesenberry indicated no relevant financial relationships.
Sophia Merchant indicated no relevant financial relationships.
Theodore Levin indicated no relevant financial relationships.
Jeffrey Fox indicated no relevant financial relationships.
Douglas Corley indicated no relevant financial relationships.
Jeffrey Lee indicated no relevant financial relationships.
Pradeep Koripella, MD1, Eshandeep Boparai, MD1, Christopher Jensen, PhD, MPH1, Jessica Badalov, MS, RDN1, Charles Quesenberry, PhD1, Sophia Merchant, MPH1, Theodore R. Levin, MD2, Jeffrey Fox, MD1, Douglas Corley, MD, PhD1, Jeffrey Lee, MD, MPH3, 46, De-Implementation of Outdated Colonoscopy Surveillance Interval Recommendations Among Patients With Low-Risk Adenomas (DESIRE), ACG 2023 Annual Scientific Meeting Abstracts. Vancouver, BC, Canada: American College of Gastroenterology.