Manasik Abdu, MD1, Mouhand FH. Mohamed, MD2, Basile Njei, MD, MPH, PhD3 1University at Buffalo-Catholic Health System, Buffalo, NY; 2Brown University, Providence, RI; 3Yale School of Medicine, New Haven, CT
Introduction: Lean Non-alcoholic fatty liver disease (NAFLD) (body mass index: BMI < 25 kg/m2) often goes undetected due to normal liver enzyme levels and the absence of diabetes. Early identification of lean NAFLD is vital for timely treatment and reducing complications. We examined the usefulness of insulin resistance (IR) in identifying NAFLD in lean individuals.
Methods: We extracted data from the National Health and Nutrition Examination Surveys (NHANES) from 2017 to 2020. Briefly, lean adults ≥ 18 years of age with valid transient elastography measurements were included, while excluding those with high alcohol consumption, viral hepatitis, or human immunodeficiency virus. Controlled attenuation parameter (CAP) ≥302 dB/m using Youden’s index defined NAFLD. IR was defined using Homeostasis Model Assessment of Insulin Resistance [HOMA-IR = insulin (μU/ml) × fasting glucose (mmol/L)/22.5]. Multivariable logistic regression analyses were performed to identify the association of HOMA-IR and other metabolic factors with NAFLD. Receiver operating characteristic (ROC) curve analysis was used to calculate the area under the ROC curve (AUC) of HOMA-IR for identification of NAFLD.
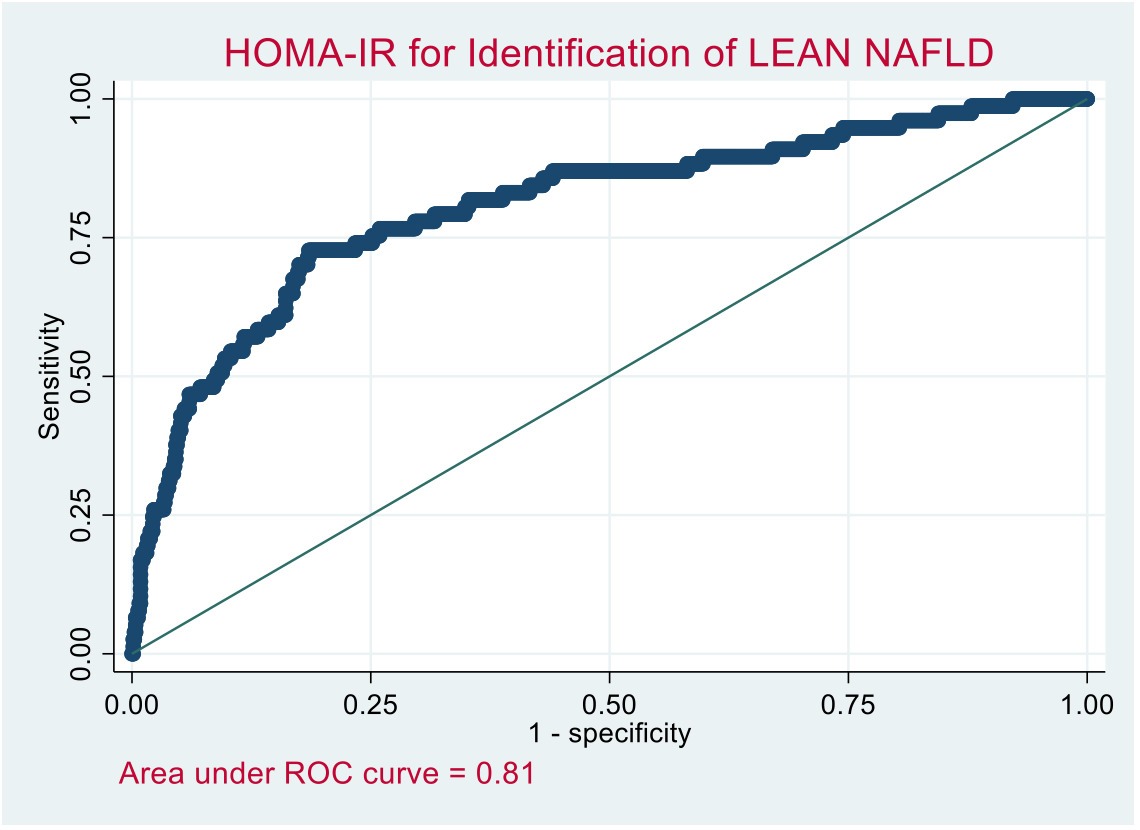
Results: A total of 860 subjects met the inclusion criteria. The median age was 53 (interquartile range 33-69 years) and 416 (48%) were women. The age-adjusted prevalence of NAFLD in lean individuals was 8.9%. We found a higher prevalence of lean NAFLD among men (9.9% vs. 7.9% in women, p < 0.01). Independent risk factors for lean NAFLD after adjusting for age, sex, race, and metabolic syndrome in a logistic regression model included: HOMA-IR > 2.0 (adjusted OR 1.40 95% CI 1.17-1.68), hemoglobin A1C (OR 1.29 95% CI 1.05-1.57), and waist circumference (OR 1.07 95% CI 1.02-1.12). The area under the curve (AUC) for HOMA-IR to predict NAFLD was 0.81(Figure 1). An optimal sensitivity of 92.2% was achieved at HOMA-IR >1.4 cut-off and a specificity of 91.6% at HOMA-IR >3.0 cut-off, with a negative predictive value of 97.8% and 93.4%, respectively. The positive predictive value remained low (< 30%) irrespective of the HOMA-IR cut-off.
Discussion: This study demonstrated that insulin resistance is a robust independent predictor of lean NAFLD and provides, albeit indirect, evidence to support the role of insulin resistance in the pathogenesis of lean NAFLD. HOMA-IR may help clinicians quickly identify lean patients without diabetes who could benefit from NAFLD screening. Yet, its low positive predictive value limits its diagnostic utility.
Figure: Figure 1: Areas under the receiver operating characteristic curve (AUC) plot of HOMA-IR (cut-off >2) for predicting NAFLD.
Disclosures:
Manasik Abdu indicated no relevant financial relationships.
Mouhand Mohamed indicated no relevant financial relationships.
Basile Njei indicated no relevant financial relationships.
Manasik Abdu, MD1, Mouhand FH. Mohamed, MD2, Basile Njei, MD, MPH, PhD3, 37, Homeostasis Model Assessment of Insulin Resistance as a Clinical Marker of Non-Alcoholic Fatty Liver Disease in Lean Individuals, ACG 2023 Annual Scientific Meeting Abstracts. Vancouver, BC, Canada: American College of Gastroenterology.