Trevor S. Barlowe, MD1, Walker D.. Redd, MD2, Angela Xue, BSPH2, Akshatha Kiran, MPH2, Justin McCallen, MD2, Swathi Eluri, MD, MSCR2, Craig C.. Reed, MD, MSCR2, Evan Dellon, MD, MPH1 1University of North Carolina, Chapel Hill, NC; 2University of North Carolina School of Medicine, Chapel Hill, NC
Introduction: Despite recommendations to perform biopsies at the time of esophageal food impaction (EFI) to evaluate for eosinophilic esophagitis (EoE), endoscopists often forgo biopsies. There are minimal data on the risks of biopsies in this setting. We aimed to determine if performing biopsies at time of esophagogastroduodenoscopy (EGD) for EFI results in complications.
Methods: We conducted a retrospective cohort study of patients who presented to UNC Hospitals from 2014-2021 with endoscopically confirmed EFI. Subjects were identified through the endoscopy reporting software using pertinent ICD codes. Demographics, clinical characteristics, EFI event details, EGD procedure details, EGD findings, complications, and pertinent outcomes were extracted from medical records then compared between those patients who did and did not undergo biopsies at time of EFI using bivariate analyses. Complications were classified as either esophageal (mucosal tear, bleeding, perforation) or extra-esophageal (aspiration, respiratory compromise, hypotension, arrhythmia).
Results: Of 188 patients who underwent EGD for EFI, 73 (39%) had biopsies. At baseline, patients who were biopsied were younger, more likely to be white, and less likely to have diabetes, GERD, or use tobacco compared to those who were not biopsied (Table 1). None of the 10 Black patients had biopsies taken. Patients with higher ASA scores, findings of impacted bone or Schatzki’s ring, and need for grasping technique were less likely to get biopsied. Those with mucosal findings or stricture suggestive of EoE were biopsied more often, but biopsies were only taken in 70% of these patients (Table 2). Of those biopsied, 47% were diagnosed with EoE. Only 2 (2.7%) of 73 biopsied patients had a complication, and neither was related to the biopsies. Patients who were biopsied were less likely to have complications (3% vs 17%; p= 0.002) or be admitted for observation (10% vs 28%; p= 0.003). There was no difference in re-admission, ICU admission, or 30-day mortality between those who were and were not biopsied.
Discussion: Esophageal biopsies at time of EFI are underperformed, as less than half of all cases, none of the Black patients, and just 70% of cases with suspected EoE had biopsies performed. While some endoscopists may worry about biopsy-associated complications, we found esophageal biopsies at time of EFI are unlikely to cause complications and therefore should be performed in the absence of extenuating circumstances.
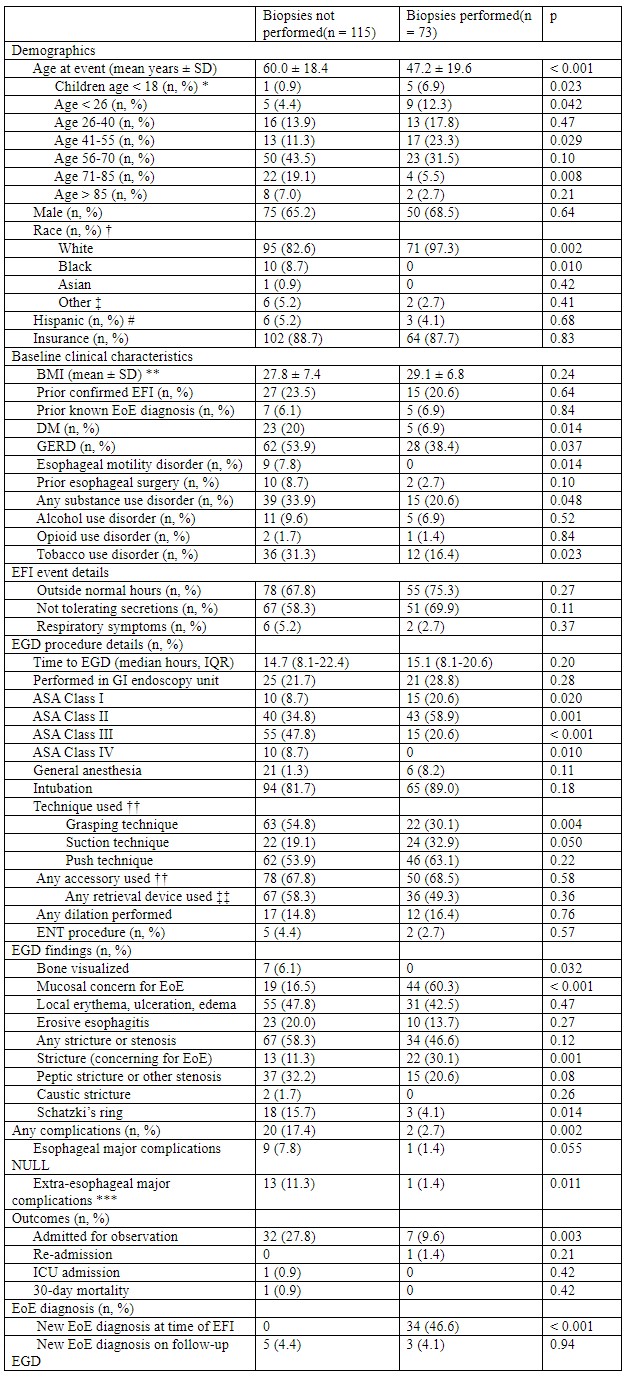
Table: Table 1: Clinical characteristics, EFI event details and outcomes for patients who did and did not get biopsies (n=188)
EFI = esophageal food impaction; SD = standard deviation; BMI = body mass index; EoE = eosinophilic esophagitis; DM = diabetes mellitus; GERD = gastroesophageal reflux disease; EGD = esophagogastroduodenoscopy; IQR = interquartile range; ASA = American society of anesthesiologists; ENT = ear, nose, and throat surgeon
*Age categories are compared to all other age categories. †Race was missing for 3 patients (race listed as “unknown” and there was no ethnicity listed). ‡Of the 8 patients with race listed as “other,” 8 had ethnicity listed as “Hispanic” and 6 had first language listed as “Spanish.” #Ethnicity was missing for 1 patient. Of the 9 patients with “Hispanic” ethnicity, 8 had race listed as “other” and 1 had race listed as “White.” **BMI was missing for 5 patients. ††For 5 patients, details about food removal, including technique, accessories used, and retrieval devices used were missing. ‡‡Retrieval devices used included biopsy forceps, non-biopsy grasping forceps, retrieval basket, loop snare, and Roth net®. NULLEsophageal major complications includes esophageal perforation, mucosal tear, or bleeding. ***Extra-esophageal major complications includes aspiration, respiratory compromise, arrhythmia, or hypotension.
Disclosures:
Trevor Barlowe indicated no relevant financial relationships.
Walker Redd indicated no relevant financial relationships.
Angela Xue indicated no relevant financial relationships.
Akshatha Kiran indicated no relevant financial relationships.
Justin McCallen indicated no relevant financial relationships.
Swathi Eluri indicated no relevant financial relationships.
Craig Reed indicated no relevant financial relationships.
Evan Dellon indicated no relevant financial relationships.
Trevor S. Barlowe, MD1, Walker D.. Redd, MD2, Angela Xue, BSPH2, Akshatha Kiran, MPH2, Justin McCallen, MD2, Swathi Eluri, MD, MSCR2, Craig C.. Reed, MD, MSCR2, Evan Dellon, MD, MPH1, 24, Performing Esophageal Biopsies During Upper Endoscopy for Esophageal Food Impaction Is Unlikely to Cause Complications, ACG 2023 Annual Scientific Meeting Abstracts. Vancouver, BC, Canada: American College of Gastroenterology.