University of Wisconsin School of Medicine and Public Health Madison, WI
Dana Ley, MD, Dmitriy Kravtsov, BS, Andrew Spiel, MD University of Wisconsin School of Medicine and Public Health, Madison, WI
Introduction: Spontaneous hyperinflation (SH) is a recognized but rare complication of intragastric balloon (IGB) placement. Urgent endoscopic removal is critical. Patients may present to centers unfamiliar with IGBs, so all gastroenterologists should be aware of this rare but dangerous complication. Specific removal kits are not always available, and in emergencies, IGBs may be removed with standard endoscopic tools.
Case Description/Methods: A 44-year-old female with obesity had an IGB placed in the Dominican Republic six months prior to presentation, with 60-pound weight loss. One week prior, she returned to the Dominican Republic. The IGB was inflated further for additional weight loss. She presents to the ED with five days of vomiting >10x/day, severe abdominal pain, and lack of bowel movements for one week. Vital signs were normal in the ED. Exam showed soft, distended abdomen, tender in the upper regions, without peritoneal signs. Labs were notable for leukocytosis of 12.0 and lipase of 422 (normal 13-60). CT abdomen/pelvis showed a large IGB (13 x 18 x 15 cm) with internal air-fluid level and no evidence of gastric outlet obstruction.
Emergent dual channel upper endoscopy (EGD) was performed. The IGB external catheter was grasped with a snare and rat-tooth forceps and pulled out of the mouth. The internal fluid was suctioned out and cultured. The IGB surface suggested microbial colonization. IGB removal was attempted with the above tools, but there was significant breakdown of the IGB, complicating removal. Two snares were used to grasp each end of the catheter, allowing for completion of IGB removal. There was a large, deep ulcer where the IGB was sitting, likely due to ischemia from the IGB. Fluid culture was negative. Bacterial culture of the IGB showed skin microbiota, and fungal culture showed rare Candida krusei. Post-procedure recovery was unremarkable; she was discharged the next day.
Discussion: SH rarely occurs post-IGB placement, and the mechanism of microbial overgrowth with hyperinflation is uncertain. Our patient had no gas-producing organisms cultured from the IGB or its fluid. If there is concern for SH, the IGB should be removed as soon as possible given risk of gastric or esophageal perforation. IGB removal is typically device-dependent and should be done following the manufacturer’s instructions, but in emergent cases, all IGBs can be aspirated with an endoscopic injection needle and removed with standard endoscopic tools.
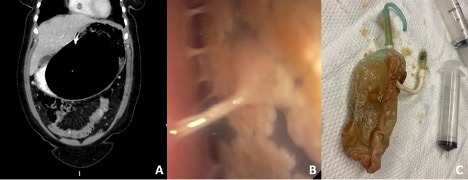
Figure: Panel A: Coronal view of patient’s CT of the abdomen/pelvis with IV and oral contrast, showing significant hyperinflation of intragastric balloon. Panel B: Endoscopic image showing intragastric balloon with appearance of internal microbial colonies and adherence to the gastric wall. Panel C: The intragastric balloon post-removal. The intragastric balloon appears to have internal microbial overgrowth. The balloon was broken during endoscopic removal, making both the internal and external catheters accessible to grasping with a snare. The entire balloon was sent for bacterial and fungal culture.
Disclosures:
Dana Ley indicated no relevant financial relationships.
Dmitriy Kravtsov indicated no relevant financial relationships.
Andrew Spiel indicated no relevant financial relationships.
Dana Ley, MD, Dmitriy Kravtsov, BS, Andrew Spiel, MD. P3735 - Removal of an Intragastric Balloon After Spontaneous Hyperinflation: A Rare Complication, ACG 2023 Annual Scientific Meeting Abstracts. Vancouver, BC, Canada: American College of Gastroenterology.