University of Kansas School of Medicine Wichita, KS
Aastha Bharwad, MD, Lawrence Zhou, MD, Stephanie J. Melquist, MD, MPH, Kyle Rowe, MD University of Kansas School of Medicine, Wichita, KS
Introduction: Cicatricial pemphigoid (CP), or benign mucous membrane pemphigoid, is a rare autoimmune blistering disorder affecting mainly the skin and mucous membranes and characterized by deposition of IgG or IgA autoantibodies and complements in the basement membrane. Esophageal involvement occurs rarely and can present years after the initial onset of disease. Our case highlights the clinical spectrum of CP and the importance to evaluate for esophageal involvement in dysphagia.
Case Description/Methods: A 75-year-old male with history of coronary artery disease, peripheral vascular disease, and hyperlipidemia presented to clinic for several weeks of unilateral left eye conjunctivitis and nine kg unintentional weight loss over the past year. He was started on polymyxin B/trimethoprim eyedrops. Labs were significant for ESR of 24 mm/hr and CRP of 0.6 mg/dL.
On clinic visit three months later, he reported progressive dysphagia to solids, with eye pain, photophobia, and blurry vision. Oral exam revealed a 2cm x 3cm beefy red irregularly shaped ulceration with several satellite lesions. These were biopsied, showing linear IgG and C3 deposition in basement membrane, consistent with CP. He was diagnosed with ocular CP and was started on prednisone and azathioprine.
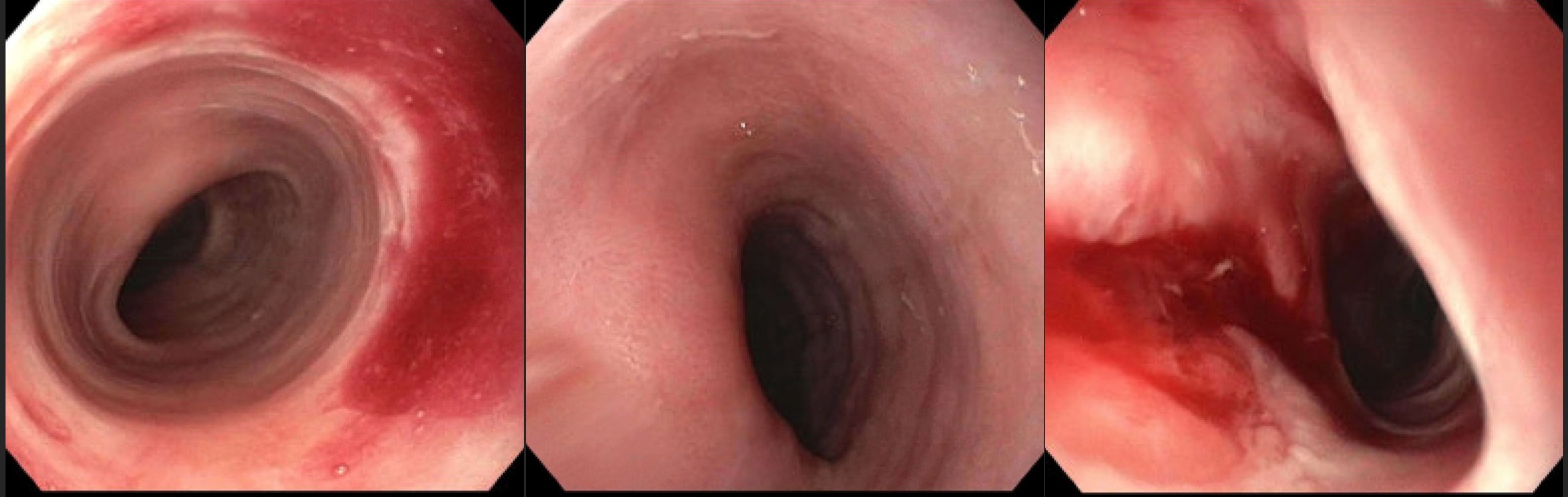
Upon follow-up one year later, the patient reported resolution of his mucosal lesions but continued to lose weight and complained of pill dysphagia. On modified barium swallow, a 13 mm barium tablet was found lodged in the mid-esophagus. Esophagogastroduodenoscopy (EGD) was then performed which showed narrow caliber esophagus with multifocal narrowing in the mid-esophagus (Figure 1,2). No mucosal sloughing was visualized; however, the patient had been on immunosuppression for the prior year with resolution of oral lesion. Savary dilation was performed with multifocal mucosal rents observed (Figure 3). Biopsies did not demonstrate changes of lymphocytic or eosinophilic esophagitis.
Follow-up EGD with repeat dilation showed expected improvement in luminal narrowing. Since index EGD, the patient has regained 2.2 kg with full resolution of his dysphagia.
Discussion: Esophageal involvement in CP can be difficult to diagnose as a cause of dysphagia when present with other causes like mouth ulcers. Majority have frank strictures and webs. Combination therapy with careful endoscopic dilatation and immunosuppression could be used for esophageal disease. Low threshold should be set for EGD in CP patients to exclude or treat those with esophageal involvement.
Figure: Figure 1: Upper third of the esophagus Figure 2: Middle third of the esophagus pre-dilation Figure 3: Middle third of the esophagus post-dilation
Disclosures:
Aastha Bharwad indicated no relevant financial relationships.
Lawrence Zhou indicated no relevant financial relationships.
Stephanie Melquist indicated no relevant financial relationships.
Kyle Rowe indicated no relevant financial relationships.
Aastha Bharwad, MD, Lawrence Zhou, MD, Stephanie J. Melquist, MD, MPH, Kyle Rowe, MD. P3341 - Esophageal Stricture in Cicatricial Pemphigoid: A Unique Case of Dysphagia, ACG 2023 Annual Scientific Meeting Abstracts. Vancouver, BC, Canada: American College of Gastroenterology.

 photo")