Session: Plenary Session 2B - Small Intestine / IBD
35 - Risankizumab Induction Therapy in Patients WIth Moderately to Severely Active Ulcerative Colitis: Efficacy and Safety in the Randomized Phase 3 INSPIRE Study
Edouard Louis, MD1, Remo Panaccione, MD2, Gareth Parkes, MD3, Laurent Peyrin-Biroulet, MD4, Marc Ferrante, MD5, Ken Takeuchi, MD, PhD6, Britta Siegmund, MD, PhD7, Phillip Levine, MD8, Jasmina Kalabic, MD9, Ezequiel Neimark, MD8, Kori Wallace, MD8, Su Chen, PhD8, W.Rachel Duan, MD8, Alessandro Armuzzi, MD10, Luc Biedermann, MD11, Edward V. Loftus, MD12, Gil Melmed, MD, MS13, Stefan Schreiber, MD14 1University Hospital CHU of Liège, Liege, Liege, Belgium; 2University of Calgary, Calgary, AB, Canada; 3Barts Health NHS Trust, London, England, United Kingdom; 4Lorraine University, Vandoeuvre, Lorraine, France; 5University Hospitals Leuven, Leuven, Liege, Belgium; 6Tsujinaka Hospital Kashiwanoha, Kashiwa, Chiba, Japan; 7Charité – Universitätsmedizin Berlin, Berlin, Berlin, Germany; 8AbbVie, North Chicago, IL; 9AbbVie Deutschland GmbH & Co. KG, Ludwigshafen, Baden-Wurttemberg, Germany; 10IRCCS Humanitas Research Hospital, Milan, Abruzzi, Italy; 11University Hospital Zürich, Zürich, Zurich, Switzerland; 12Mayo Clinic College of Medicine and Science, Rochester, MN; 13Center for Inflammatory Bowel Diseases, Cedars-Sinai Medical Center, Los Angeles, CA; 14University Hospital Schleswig-Holstein, Kiel, Schleswig-Holstein, Germany
Introduction: Risankizumab (RZB), a monoclonal antibody neutralizing interleukin (IL)-23p19, was evaluated for efficacy and safety of induction therapy in patients with moderately to severely active ulcerative colitis (UC) in a large phase 3 trial, INSPIRE (NCT03398148).
Methods: Eligible patients (18-80 years) with moderately to severely active UC (Adapted Mayo score of 5–9 points) and an endoscopic subscore of 2-3 (per central review) were enrolled. Patients were required to have a diagnosis of UC for at least 3 months prior to baseline, and demonstrated intolerance or inadequate response to conventional and/or advanced therapies (biologics, JAK inhibitors, and S1P receptor modulators). Patients (N=975) were randomized 2:1 to receive either RZB 1200 mg intravenously (IV) or placebo (PBO) at Weeks (Wks) 0, 4, and 8. The primary endpoint was clinical remission (per Adapted Mayo score) at Wk 12 (see Figure legend for definitions). Key, ranked secondary endpoints included clinical response, endoscopic improvement, endoscopic remission, histologic-endoscopic mucosal improvement (HEMI), and histologic-endoscopic mucosal remission (HEMR), which were measured at Wk 12, unless otherwise noted.
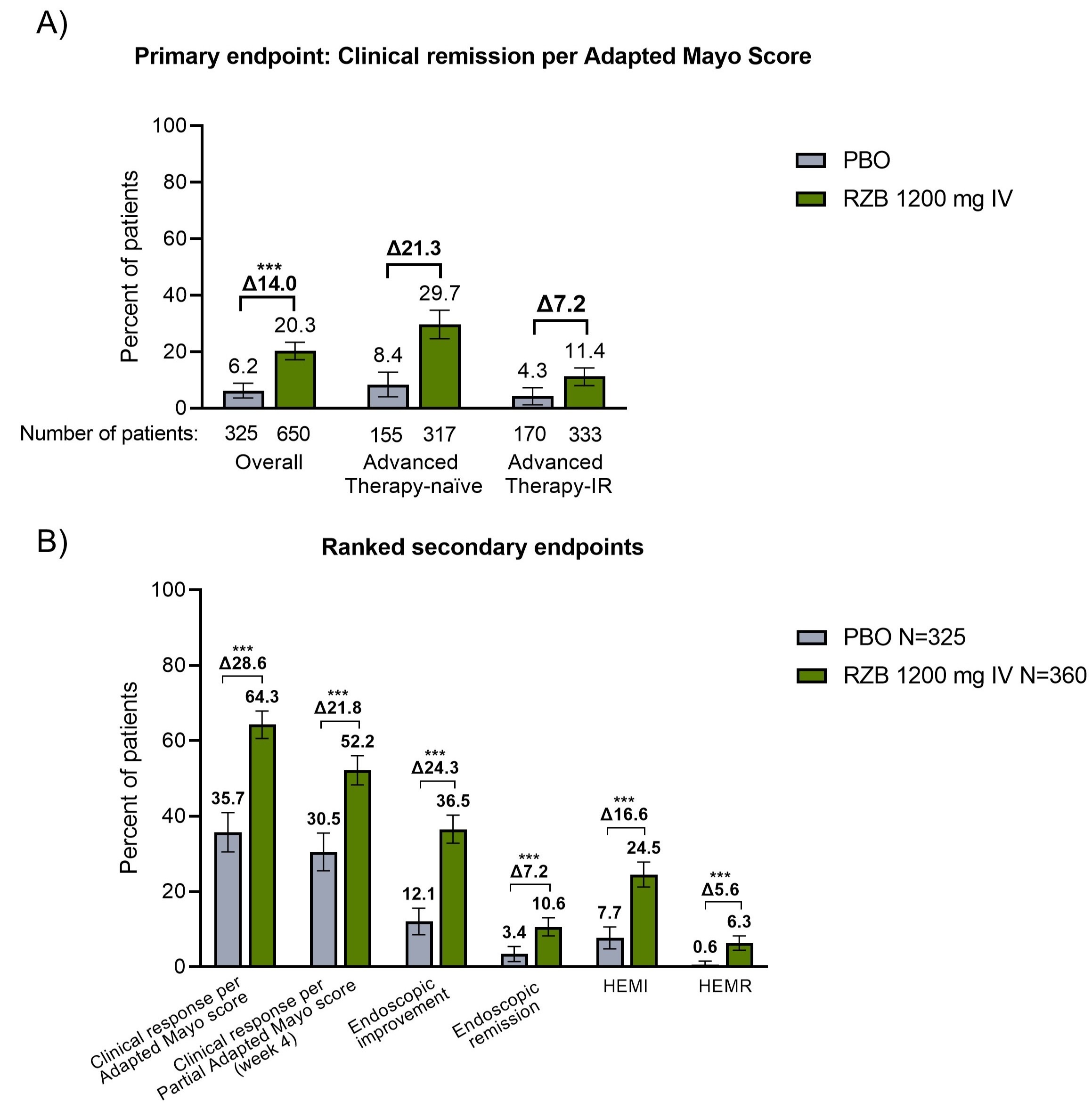
Results: Baseline characteristics were similar between treatment groups. Significantly more patients receiving RZB achieved clinical remission vs PBO (20.3% vs 6.2%, adjusted treatment difference 14.0% [95% CI, 10.0%-18.0%], P< .00001, Figure 1A). All ranked secondary endpoints were met. RZB attained higher rates of clinical response (per Adapted Mayo score at Wk 12 and per Partial Adapted Mayo score at Wk 4), endoscopic improvement, endoscopic remission, HEMI, and HEMR, compared to PBO (P< .00001 for all endpoints, Figure 1B). Adverse event (AE) rates were 42.1% in RZB vs 49.7% PBO, serious AEs (2.3% vs 10.2%), severe AEs (2.5% vs 10.2%), AEs leading to discontinuation of study drug (0.6% vs 3.7%), and serious infections (0.6% vs 1.2%) were numerically lower in the RZB arm. No adjudicated major adverse cardiovascular events, adjudicated anaphylaxis, or serious hepatic events were reported. One death occurred in the RZB group due to COVID-19 pneumonia.
Discussion: In patients with moderately to severely active UC, RZB was superior to PBO as an induction therapy for clinical remission and all secondary clinical, endoscopic, and endoscopic-histologic endpoints. RZB was well-tolerated, and no new safety risks were observed.
Figure: Figure 1. Primary and Key Secondary Endpoints All patients in this dataset were included here within the ITT population. Endpoints were assessed at Week 12 unless otherwise noted. Clinical Remission per Adapted Mayo score: Stool frequency subscore ≤ 1 and not greater than baseline, rectal bleeding subscore of 0, and endoscopic subscore ≤ 1 without friability Clinical Response per Adapted Mayo: Decrease from baseline ≥ 2 points and ≥ 30%, in addition to a decrease in RBS ≥ 1 or an absolute rectal bleeding score (RBS) ≤ 1 Clinical Response per Partial Adapted Mayo: Decrease from baseline ≥ 1 point and ≥ 30% a decrease in RBS ≥ 1 or an absolute RBS ≤ 1 Endoscopic Improvement: Endoscopic subscore of 0 or 1 without friability Endoscopic Remission: Endoscopic subscore = 0 Histologic-Endoscopic Mucosal Improvement (HEMI): Endoscopic subscore of 0 or 1 without friability and Geboes score ≤ 3.1 Histologic-Endoscopic Mucosal Remission (HEMR): Endoscopic subscore of 0 and Geboes score < 2.0 Results were stratified by baseline corticosteroid use (yes vs no), baseline Adapted Mayo score (≤ 7 vs > 7), and the number of advanced therapy failures (0, 1, >1). Results are based on non-responder imputation incorporating multiple imputation (NRI-MI) to handle missing data due to COVID-19 or due to geopolitical conflict in Ukraine or surrounding areas. ***P-value <.00001 vs PBO. P-value for treatment difference between RZB 1200 mg IV and PBO, using Cochran-MantelHaenszel (CMH) test for categorical endpoints, controlling for stratification factors. IR, inadequate response
Stefan Schreiber: AbbVie – Personal fees. Amgen – Personal fees. Arena Pharmaceuticals – Personal fees. Biogen – Personal fees. Bristol Myers Squibb – Personal fees. Celgene – Personal fees. Celltrion Healthcare – Personal fees. Dr. Falk Pharma – Personal fees. Eli Lilly – personal fees. Ferring Pharmaceuticals – personal fees. Fresenius Kabi – Personal fees. Galapagos – Personal fees. Gilead – Personal fees. Hikma Pharmaceuticals – Personal fees. I-Mab – Personal fees. Janssen Pharmaceuticals – Personal fees. Morphic – Personal fees. MSD – Personal fees. Mylan – Personal fees. Pfizer – Personal fees. Protagonist – Personal fees. ProventionBio – Personal fees. Sandoz/Hexal – personal fees. Takeda – Personal fees. Theravance Biopharma – Personal fees. UCB – personal fees.
Edouard Louis, MD1, Remo Panaccione, MD2, Gareth Parkes, MD3, Laurent Peyrin-Biroulet, MD4, Marc Ferrante, MD5, Ken Takeuchi, MD, PhD6, Britta Siegmund, MD, PhD7, Phillip Levine, MD8, Jasmina Kalabic, MD9, Ezequiel Neimark, MD8, Kori Wallace, MD8, Su Chen, PhD8, W.Rachel Duan, MD8, Alessandro Armuzzi, MD10, Luc Biedermann, MD11, Edward V. Loftus, MD12, Gil Melmed, MD, MS13, Stefan Schreiber, MD14, 35, Risankizumab Induction Therapy in Patients WIth Moderately to Severely Active Ulcerative Colitis: Efficacy and Safety in the Randomized Phase 3 INSPIRE Study, ACG 2023 Annual Scientific Meeting Abstracts. Vancouver, BC, Canada: American College of Gastroenterology.